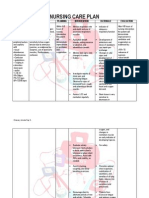
Assessment Diagnosis Planning Implementation Rationale Evaluation
Assessment Diagnosis Planning Implementation Rationale Evaluation
Download as doc, pdf, or txt
You might also like
- Copd NCPDocument16 pagesCopd NCPSuperMaye100% (1)
- Nursing Care Plan - Pulmonary EmbolismDocument3 pagesNursing Care Plan - Pulmonary EmbolismPui_Yee_Siow_6303100% (10)
- SCIQuestions CaseStudyKeyDocument4 pagesSCIQuestions CaseStudyKeyDeez NutsNo ratings yet
- NCP FORM For TetralogyDocument3 pagesNCP FORM For TetralogyGraceMelendres100% (3)
- Tuberculosis Nursing Care Plan - Ineffective Airway ClearanceDocument2 pagesTuberculosis Nursing Care Plan - Ineffective Airway ClearanceCyrus De Asis86% (36)
- Hypovolemic Shock Case StudyDocument6 pagesHypovolemic Shock Case StudyJenn GallowayNo ratings yet
- Liberation From Mechanical VentilationDocument21 pagesLiberation From Mechanical VentilationRins Chacko50% (2)
- Decreased Cardiac OutputDocument9 pagesDecreased Cardiac OutputChinita Sangbaan75% (4)
- NCP Pleural EffusionDocument7 pagesNCP Pleural EffusionEjie Boy Isaga100% (2)
- PharmacologyDocument13 pagesPharmacologyCARTAGENA1100% (20)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Cardiac ComplicationDocument12 pagesCardiac ComplicationResa ShotsNo ratings yet
- Risk For AspirationDocument9 pagesRisk For AspirationFerreze AnnNo ratings yet
- Nursing Management of BurnDocument40 pagesNursing Management of BurnSalinKaur0% (1)
- Renal Failure Nursing Care PlanDocument2 pagesRenal Failure Nursing Care Planemman_abz33% (3)
- NCP Eclampsia 1Document2 pagesNCP Eclampsia 1Thesa FedericoNo ratings yet
- NCP-Case Presentation (CHF)Document4 pagesNCP-Case Presentation (CHF)Jessamine EnriquezNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanAdreanah Martin RañisesNo ratings yet
- NCP IcuDocument12 pagesNCP IcuHazel Palomares50% (2)
- Assessment Diagnosis Rationale Planning Interventions Rationale EvaluationDocument3 pagesAssessment Diagnosis Rationale Planning Interventions Rationale EvaluationJharene BasbañoNo ratings yet
- Mary Cris Canon CHF For or Case Study.Document12 pagesMary Cris Canon CHF For or Case Study.Mary Cris CanonNo ratings yet
- Most Common Nursing Care Plans (1)Document96 pagesMost Common Nursing Care Plans (1)rn.nursetomlinsonNo ratings yet
- Ncp'sDocument8 pagesNcp'sDuchess Kleine RafananNo ratings yet
- Care Plan Designed For Mr. SalmanDocument2 pagesCare Plan Designed For Mr. SalmanHouda HayekNo ratings yet
- LUNGcancer NCPregieDocument1 pageLUNGcancer NCPregieShermay MortelNo ratings yet
- ABCDE Approach, Resus - Org.ukDocument7 pagesABCDE Approach, Resus - Org.ukMohamed NasrAllahNo ratings yet
- NCP PleuralDocument5 pagesNCP Pleuraljanine_valdezNo ratings yet
- Assessment of Cardiovascular SystemDocument5 pagesAssessment of Cardiovascular SystemAnamika ChoudharyNo ratings yet
- Nursing Care PlanDocument28 pagesNursing Care PlanChristine Karen Ang Suarez67% (3)
- Foundations Exam 3Document25 pagesFoundations Exam 3TeNo ratings yet
- NCLEX Day 1Document17 pagesNCLEX Day 1jasonNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- Done - Skills LectureDocument31 pagesDone - Skills LectureMeryl RamosNo ratings yet
- Mechanical VentilationDocument42 pagesMechanical VentilationWiz SamNo ratings yet
- The Main Principles:: A B C D EDocument4 pagesThe Main Principles:: A B C D EHatem FaroukNo ratings yet
- NCP'SDocument10 pagesNCP'SEjie Boy IsagaNo ratings yet
- NCPDocument15 pagesNCPCamille PinedaNo ratings yet
- Ineffective Breathing PatternDocument8 pagesIneffective Breathing PatternJansen Arquilita Rivera100% (2)
- Postpartum HemorrhageDocument3 pagesPostpartum HemorrhageClaire Canapi BattadNo ratings yet
- NANDA DefinitionDocument5 pagesNANDA DefinitionAngel_Liboon_388No ratings yet
- Impaired Gas ExchangeDocument4 pagesImpaired Gas ExchangeNuraini Hamzah100% (1)
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- Nursing Care Plan: Hanoi Medical University Advanced Nursing ProgramDocument11 pagesNursing Care Plan: Hanoi Medical University Advanced Nursing Programlephuongloan2601No ratings yet
- A B C D e AssessmentDocument6 pagesA B C D e AssessmentANGELICA JANE FLORENDONo ratings yet
- Nursing Care PlanDocument26 pagesNursing Care PlanPrincessLienMondejarNo ratings yet
- The ABCDE ApproachDocument8 pagesThe ABCDE ApproachAsmaa TahaNo ratings yet
- AH Final Exam Review - FINALDocument19 pagesAH Final Exam Review - FINALRin noharaNo ratings yet
- Elevated Blood PressureDocument3 pagesElevated Blood PressureSean MercadoNo ratings yet
- NCP For Acute Coronary SyndromeDocument3 pagesNCP For Acute Coronary Syndromesarahtot60% (5)
- Interventions For Critically Ill Patients With Respiratory Problems HandoutsDocument115 pagesInterventions For Critically Ill Patients With Respiratory Problems HandoutsDemuel Dee L. BertoNo ratings yet
- Oxy Act 2Document5 pagesOxy Act 2Joshua DauzNo ratings yet
- Abcde Erp39p44Document6 pagesAbcde Erp39p44Elizabeth Toapanta VrnNo ratings yet
- NCP Ineffective Gas ExchangeDocument2 pagesNCP Ineffective Gas ExchangeRez ApegoNo ratings yet
- Nursing DiagnosisDocument16 pagesNursing DiagnosisSi Bunga JonquilleNo ratings yet
- Segui NCPDocument4 pagesSegui NCPRichelle TalaguitNo ratings yet
- عناية م 4Document85 pagesعناية م 4tbtv5wnm9jNo ratings yet
- NCPDocument9 pagesNCPTracy Camille EscobarNo ratings yet
- Nursing Diagnosis Analysis Goal & Objectives Nursing Intervention Rationale EvaluationDocument2 pagesNursing Diagnosis Analysis Goal & Objectives Nursing Intervention Rationale EvaluationLP BenozaNo ratings yet
- Approach To An Unconscious Patient-OyeyemiDocument41 pagesApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument14 pagesAssessment Diagnosis Planning Implementation Rationale EvaluationJennifer ArdeNo ratings yet
- AssessmentDocument1 pageAssessmentJennifer ArdeNo ratings yet
- Y Cy Y !"#$Y %!"#$Y & &' (Y + (,YYDocument5 pagesY Cy Y !"#$Y %!"#$Y & &' (Y + (,YYJennifer ArdeNo ratings yet
- NURSING CARE PLAN - SuicidalactDocument4 pagesNURSING CARE PLAN - SuicidalactJennifer ArdeNo ratings yet
- Pathophysiology of ThrombophlebitisDocument3 pagesPathophysiology of ThrombophlebitisJennifer ArdeNo ratings yet
- AdverbDocument1 pageAdverbJennifer ArdeNo ratings yet
- A04 PDFDocument16 pagesA04 PDFQueen JazNo ratings yet
- Congestive Heart Failure: Dr. J. SaravananDocument31 pagesCongestive Heart Failure: Dr. J. Saravananpetervazhayil100% (1)
- Spots 2Document17 pagesSpots 2ashok kalyaniNo ratings yet
- Sdi 2011Document311 pagesSdi 2011Mohammed Ahmad Al-MuhurNo ratings yet
- DIGOXINDocument19 pagesDIGOXINDedeSumantraNo ratings yet
- Intravenous Antibiotics Diagnostic Tests Urinalysis Sputum CultureDocument18 pagesIntravenous Antibiotics Diagnostic Tests Urinalysis Sputum CultureJennifer ChuaNo ratings yet
- Pharmacology Notes NursingDocument25 pagesPharmacology Notes NursingKyle Marks100% (6)
- PharmacologyDocument88 pagesPharmacologyالدنيا ساعة فاجعلها طاعة100% (2)
- Cardiac Surgery - Postoperative ArrhythmiasDocument9 pagesCardiac Surgery - Postoperative ArrhythmiaswanariaNo ratings yet
- NCLEX Select All That Apply Practice Exam 4Document8 pagesNCLEX Select All That Apply Practice Exam 4Heather ClemonsNo ratings yet
- Pharma La La La LaDocument32 pagesPharma La La La LaAndie AlbinoNo ratings yet
- Hypokalemia ReportDocument9 pagesHypokalemia Reportarah006No ratings yet
- SET-J RespReviewResults 20231017 155722Document14 pagesSET-J RespReviewResults 20231017 155722Erika Jane PurificacionNo ratings yet
- Cardiovascular Pharmacology ConceptsDocument11 pagesCardiovascular Pharmacology ConceptsHuney Kumar100% (1)
- Cardiac PoisonsDocument36 pagesCardiac PoisonsTARIQNo ratings yet
- Compilation of QuizzesDocument10 pagesCompilation of QuizzesElesis samaNo ratings yet
- Chapter-5 - Unit-1 - Pharmacognosy: LaxativesDocument9 pagesChapter-5 - Unit-1 - Pharmacognosy: LaxativesAaQib Ali RaZaNo ratings yet
- Pharma Moments: Antianxiety/Sedatives Minor TranquilizersDocument3 pagesPharma Moments: Antianxiety/Sedatives Minor TranquilizersTita MonzalesNo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Pharmacology Exam 4 ReviewDocument8 pagesPharmacology Exam 4 ReviewAnonymous 0Yvbef1xNo ratings yet
- 715 PrometricDocument61 pages715 PrometricNosheen HaqNo ratings yet
- Usp DizolvareDocument168 pagesUsp Dizolvaremelania.irimiaNo ratings yet
- Drugs in CHFDocument48 pagesDrugs in CHFBishnu BhandariNo ratings yet
- Respiratory and Cardiovascular Drugs TestDocument10 pagesRespiratory and Cardiovascular Drugs TestMaria Chrislyn Marcos GenorgaNo ratings yet
- Drug InteractionsDocument33 pagesDrug Interactions88AKK100% (1)
- 12 Drugs Acting On The Cardiovascular SystemDocument7 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- 2.20140209 Question PaperDocument16 pages2.20140209 Question PaperdrpnnreddyNo ratings yet
- Domingo, Precious Mae TDocument56 pagesDomingo, Precious Mae Tbevzie datuNo ratings yet
- Board Exam Nursing Test III NLE With AnswersDocument12 pagesBoard Exam Nursing Test III NLE With AnswersRaymark Morales100% (2)